Community paramedicine and mobile integrated healthcare (MIH) programs do a lot of work that traditional 911 documentation was never designed to capture.
It’s not just one incident. It’s the phone call two days later, the follow-up visit, the medication adjustment, the benefits paperwork—all the in-between touches that actually move the needle for a patient over time.
That’s why technology matters.
You can have the right mission and the right team, but if the documentation and reporting don’t match the work, it becomes hard to scale. Hard to measure. And hard to show value to partners and stakeholders.
In the short demo below, ImageTrend Sales Engineer Gabe Schultz walks through what ImageTrend’s Community Health module inside the Elite platform looks like day-to-day, starting with the patient record, then moving into programs, impact scoring, visit documentation, and worksheets.
A Closer Look at the Community Health Module
Start with the Patient Record, Not the Incident
A community health program lives or dies on continuity.
Community-based care isn’t built around a single 911 response. It’s built around patterns, follow-ups, and long-term engagement. That’s why the foundation is the patient record, not the incident report.
The patient record is where teams capture more than demographics and medical history. It’s where they store documents that providers may need in the field, where enrollment details live, and where information persists beyond a single visit.
From there, three areas become especially important for community paramedicine and MIH workflows:
Community Health tab
This is where agencies can see the programs a patient is involved in and the broader “journey” they’ve had with your organization, including past enrollments, completed programs, and ongoing work.
Contact history (the longitudinal view)
This is the “crux” of the longitudinal view in the module. It brings together what’s happening on the 911 side and what’s happening inside the community health program; you can see interactions in chronological order and understand who has engaged with the patient, when, and why.
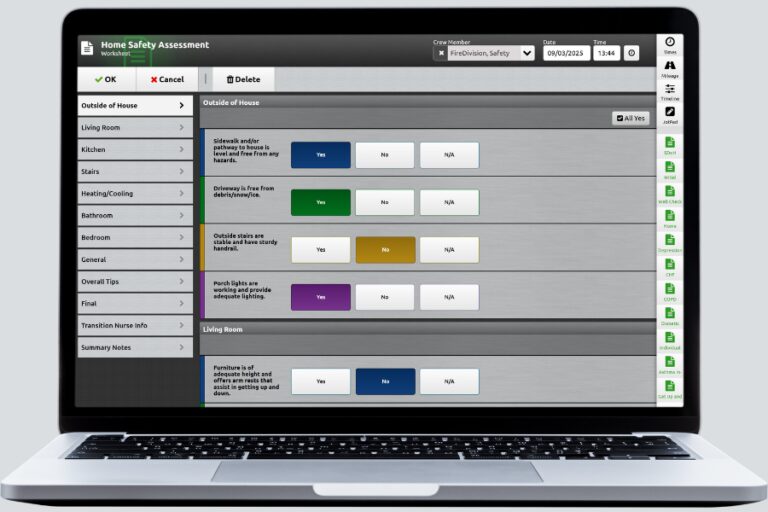
Worksheets
Worksheets support structured data collection that’s specific to the work you’re doing with a given patient, especially when you need consistency across a program or a standard checklist for enrollment.
This is where community health documentation starts to feel less like “charting” and more like case management over time. It’s the shift many MIH teams are trying to make as their programs mature.
Define Your Community Health Programs and Keep Enrollment Organized
Community health programs aren’t one-size-fits-all. One agency may focus heavily on high utilizers. Another may need fall prevention, opioid prevention, behavioral health outreach, or chronic disease support.
Programs function as the organizing framework behind those efforts. They allow agencies to group patients by initiative, align interventions to specific goals, and track participation over time. Instead of managing scattered notes and disconnected visits, teams can clearly see who is enrolled in what and why.
That structure matters for daily operations, but it also matters for accountability.
If your program is expected to show impact, whether to hospital partners, municipal leadership, or grant stakeholders, clean enrollment and reporting architecture become essential. You need to demonstrate trends. Stakeholders want to see clear trends, measurable progress, and outcomes they can quantify.
Measurement and outcome reporting are foundational to community paramedicine and MIH sustainability. Reports and dashboards should make it possible to track:
- Changes in patient risk levels
- Utilization patterns
- Interventions delivered
- Operational impact
- Specific program KPIs
Without organized programs and structured enrollment, that level of visibility becomes difficult to maintain.
Identify High-Risk and High-Utilizer Patients with Impact Score™
A lot of community paramedicine teams already know their “frequent flyers.”
But identifying emerging risk early is a different challenge, especially when call volume is rising and crews are stretched thin.
That’s where Impact Score comes in.
Impact Score analyzes recent utilization patterns and incident frequency using data agencies already collect. By weighting those data elements, it helps surface patients whose utilization is trending upward, even if they haven’t yet crossed a formal “high utilizer” threshold.
That visibility creates an opportunity for earlier outreach. Instead of waiting for the fourth call in 30 days, teams can intervene while patterns are still forming.
This is the difference between a program that is constantly reacting, and one that is intentionally proactive.
In practice, that shift can produce measurable results. For example, West Allis Fire Department’s MIH program reduced high-utilizer calls from an average of 25–28 per month to approximately 5.3 per month, about an 80% reduction.
Document Visits the Way Your Program Actually Works
Once patients are identified and enrolled, the real work begins: home visits, follow-ups, assessments, and ongoing coordination.
The visit form is designed to reflect how community health teams actually operate. If you’re familiar with Elite ePCR configurability, that same flexibility carries over here.
Form layouts, validation rules, supplemental questions, and visibility settings can all be configured so the workflow aligns with how your program functions in the field. Instead of forcing providers into a rigid template, the documentation supports the care model you’ve built.
The platform also includes AI Assist capabilities that many teams already use on the ePCR side, such as OCR-style document scanning and talk-to-text narrative functionality.
For most community health programs, this isn’t about adding more technology. It’s about removing friction so providers can spend less time typing and more time focused on the patient.
Use Worksheets to Standardize Care Without Making it Rigid
Worksheets play an important role in creating consistency across a community health program.
They can support specific assessments (such as an opioid-related screening) guide required program steps, or serve as structured enrollment checklists that ensure every patient receives the same baseline process.
In addition to single-visit assessments, patient worksheets can continue over time. That allows teams to track progress across multiple visits and weeks, instead of treating each interaction as a standalone event.
This is often what programs mean when they say they want “consistency.” Not cookie-cutter care. Just a workflow that’s reliable, trackable, and easier to sustain.
Why This Matters for MIH and Community Paramedicine Teams
Community-based care is expanding. Expectations are rising. And more programs are being asked to prove their value—whether that’s reduced low-acuity 911 calls, improved outcomes, better continuity of care, or clearer reporting to partners and stakeholders.
The work itself isn’t new. But the pressure to measure it, scale it, and sustain it is.
The right technology doesn’t replace clinical expertise or community relationships. It supports them. It provides structure behind the outreach, visibility into patterns over time, and a way to show that proactive care is making a difference.
Want to talk through your program goals and workflows? Speak with one of our Community Health experts to explore how the platform can support your MIH initiatives.

Teagan Fast
Optional Pre-Title H3 – Basic Content on White
Paragraph Text – Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat.