About this Research Project
Authors: Alissa Morrison, BAS, Paramedic1, Macall Leslie Salewon, MPH2, Jonathan Powell, PhD, NRP2, Morgan K. Anderson, MPH, FAEMS2
1Bureau of Emergency Preparedness, EMS and Systems of Care, Michigan Department
of Health & Human Services
2Clinical and Research Services, ImageTrend, LLC
Background
Motor vehicle collisions (MVC) remain a leading cause of injury and death in the United States. Entrapped patients are at a higher risk of significant injury than patients who are not. Recent studies have outlined clinical recommendations for treatment of entrapped patients including airway management and patient experience as well as safety implications for first responders on scene and best practices for performing the extrication itself. There remains a need for studies to compare the characteristics and prehospital care patterns of 9-1-1 responses for MVCs between those with and without patient extrication at the national level.
Objective
The primary goal of this study was to compare characteristics of patients and prehospital care in MVC with and without documented extrication.
Methods
Study Inclusion Criteria:
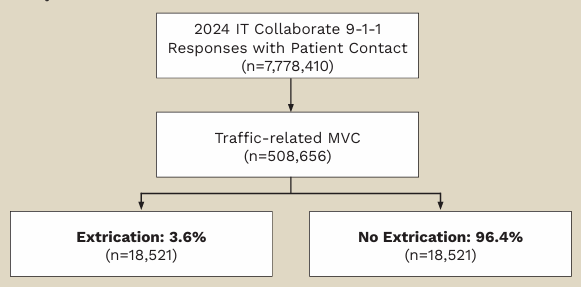
- Pedestrian, pedal cyclist, and non-traffic MVC excluded to minimize potential differences in extrication methods required.
- Extrication was identified based on documentation in either NEMSIS eInjury.04 (Trauma Triage Criteria) or eResponse.10 (Type of Scene Delay).
Study Statistics:
- Descriptive statistics (n, %) and chi-square test were used to assess differences in patient demographics, clinical status, and prehospital care provided by extrication status.
- Distribution of key response times (time to first vital sign measurement, first airway procedure, and total time on scene) by extrication status were compared (median, interquartile range).
- Stata 19 MP was used for all analyses.
Figure 1. Medications Administered by EMS by Extrication Status

Figure 2. Procedures Used by EMS by Extrication Status

Figure 3. Distribution of Key Response Times from EMS Arrival in MVC by Extrication Status
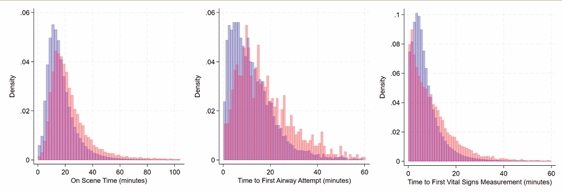
Difference in median time interval between MVCs with & without extrication:
- Time to first measured vital sign: 2.1 minutes longer
- Time to first airway: 4.7 minutes longer
- Overall time on scene: 5 minutes longer
Conclusions
Patients in MVC that required extrication were in worse clinical condition and required higher levels of prehospital clinical intervention than those in MVC without extrication. Furthermore, time to initiate key assessment and resuscitation procedures took longer, as well as total time on scene. It is possible that some clinicians may document extrication exclusively in the narrative, which would limit their capture in this study due to the lack of narrative availability in the dataset. This may contribute to the lower prevalence of MVC extrications in this study compared to other estimates. Overall, while less than 5% of MVC in this national cross-section of 9-1-1-responses had extrication documented, patterns of care, additional scene time and increased transport for these patients indicate a subset with high prehospital resource utilization.