About this Research Project
Authors: Morgan K. Anderson1, Jonathan R. Powell1, Christopher B. Gage2, Hannah Yang3, Eliza Little4, Anne Vossbrink5, Peter Geissert6, Felicia Alvarez7, Amber Viitanen8, Doug Taylor9, Lance Iversen10, Jay Otsby11, Chad Pore12
1Clinical & Research Services, ImageTrend Inc; 2National Registry of EMT’s; 3EMS, Trauma Systems, and Injury Prevention, Montana Dept. of Public Health & Human Services; 4Office of Emergency Medical Services, Connecticut Department of Public Health; 5Bureau of EMS and Trauma System, Arizona Dept. of Health Services; 6Oregon Emergency Medical Services Program, Oregon Health Authority; 7Bureau of EMS, Utah Dept, of Public Safety; 8Emergency Medical & Trauma Services, Colorado Department of Public Health & Environment; 9Kentucky Board of Emergency Medical Services; 10Office of EMS & Trauma, South Dakota Dept. of Health; 11Office of Emergency Medical Services, Wyoming Dept. of Health; 12Kansas Board of EMS
Importance
Interfacility transports (IFT) are a critical yet underexamined element of the emergency healthcare continuum, enabling timely transitions to higher levels of care for patients with complex medical or traumatic conditions. These transports—performed by emergency medical service (EMS) clinicians—occur via air transport (AT) and ground transport (GT) services, depending on acuity, geography, and available resources. As EMS systems across the U.S. face growing workforce shortages and operational strain, a comprehensive understanding of IFT patterns is essential. Enhanced insight into transport modality, frequency, and clinical indication can inform policy, support targeted workforce development, and promote more efficient deployment of EMS assets.
Objective
Describe the utilization of EMS AT vs. GT for hospital-to-hospital IFT.
Methods
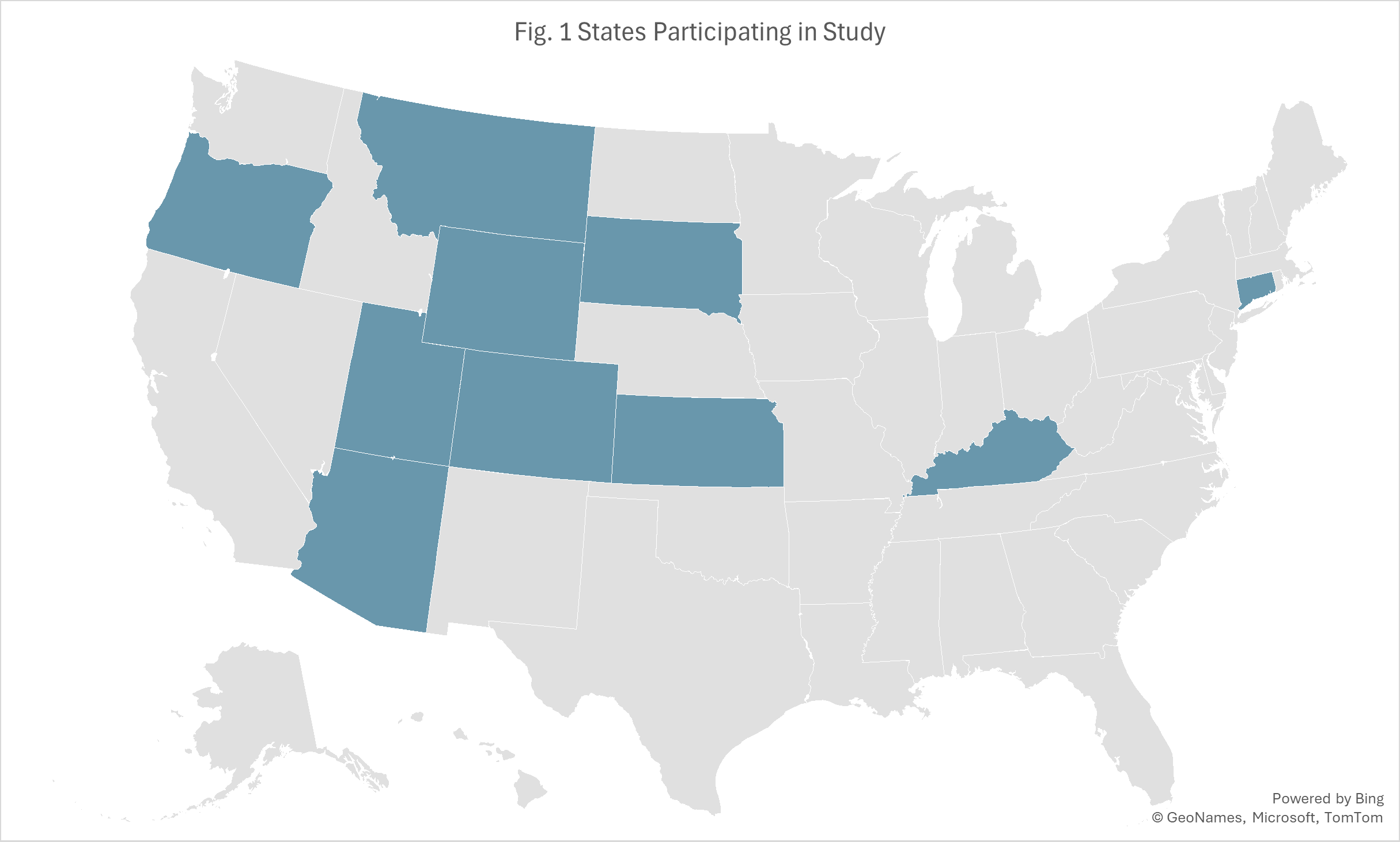
We conducted a retrospective observational analysis of ten U.S. states—Arizona, Colorado, Connecticut, Kansas, Kentucky, Montana, Oregon, South Dakota, Utah, and Wyoming—for the year 2024. Hospital-to-Hospital IFT was identified utilizing scene location type (eScene.09) and type of destination (eDisposition.21) from standardized EMS records using the ImageTrend Elite Platform. We compared AT and GT modalities using descriptive statistics to identify patient demographics, incident characteristics, and EMS care delivery. Analyses included initial patient vitals (Glasgow coma total score, systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate, respiratory rate, and pulse oximetry), as well as the top 10 documented medications and procedures administered during transport.
Results
Of 463,628 IFTs analyzed, 72,397 (16%) were AT and 391,231 (84%) were GT. Characteristics for patients transported by AT and GT were similar for sex (male: AT-52.3% vs. GT-51.2%), but differences were noted in pediatric ≤1 year (6.3% vs. 3.3%), white race (51.3% vs. 67.7%), missing race (22.4% vs. 9.8%), and non-metro incident location (53.2% vs. 20.7%). While scene location and destination type indicated hospital-to-hospital transfers, 7.4% of AT and 12.1% of GT had a service request of 9-1-1 response.
Significant differences were noted in the primary impressions observed between AT and GT, including neurological (18.0% vs. 8.7%), cardiovascular (15.7% vs. 9.9%), injury/trauma (10.7% vs. 6.3%), and mental health (0.6% vs. 8.0%) rates. Documented medications and procedures had large variability between modalities. The top three medications documented for overall IFTs were oxygen (28.4% vs. 10.2%), fentanyl (22.0% vs. 2.5%), and ondansetron (10.4% vs. 2.1%). The top three procedures were cardiac 3/4/5 lead echocardiogram (ECG) (31.2% vs. 19.3%), patient assessment (0.1% vs. 16.2%), and contacting medical control (29.0% vs. 4.7%).
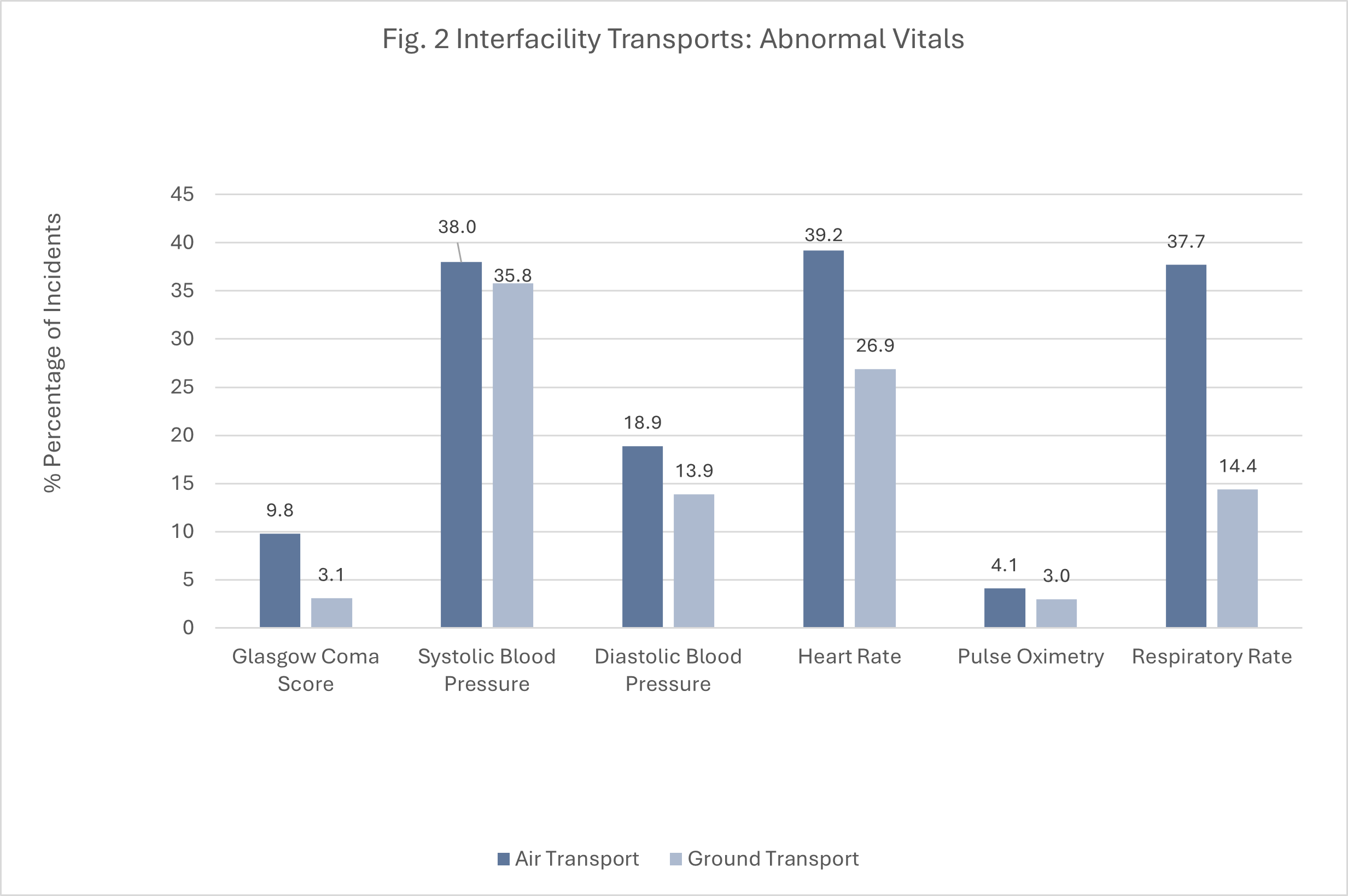
Air IFT had a higher proportion of incidents with documented severe GCS (6.0% vs. 1.3%), abnormal SBP (38.0% vs. 35.8%), abnormal DPB (18.9% vs. 13.9%), abnormal heart rate (39.2% vs 26.9%), abnormal pulse oximetry (4.1% vs. 3.0%), and abnormal respiratory rate (37.7% vs 14.4%).
Conclusion
Although all included transports met criteria for hospital-to-hospital transfers, 7.4% of air and 12.1% of ground interfacility transports were associated with a 9-1-1 service request type. This finding may reflect variation in dispatch protocols, operational workflows, or state-level coding practices. Air transports were more commonly associated with higher-acuity cases—defined by abnormal vital signs, a greater frequency of medications administered, and more procedures performed—and were more likely to occur in non-metro areas. These patterns highlight the essential role of air transport in supporting access to advanced care across geographically dispersed regions and underscore the need for further research into EMS triage, transport decision-making, and interfacility coordination to optimize resource use and ensure equitable patient care.